Question
How do I repair over-exfoliated skin?
Quick Answer
The repair almost always starts by doing less, not by buying another product. Stop using all exfoliating acids, scrubs, peel pads, retinoids, strong vitamin C, fragranced toners, and anything that stings, and let the skin run on a gentle cleanser, a bland moisturizer, and a tolerable sunscreen until ordinary products feel normal again. Look for ingredients such as ceramides, glycerin, panthenol, niacinamide, petrolatum, and colloidal oatmeal in moisturizers, applied to slightly damp skin. Most surface comfort returns over several days to a couple of weeks of that simplified routine, with lingering tone, fine flaking, and dark marks taking longer. Spreading rash, swelling, hives, oozing, blistering, eye-area symptoms, severe pain, or anything that does not start improving once actives are paused belongs with a dermatologist rather than another barrier serum.
What over-exfoliated skin usually looks like
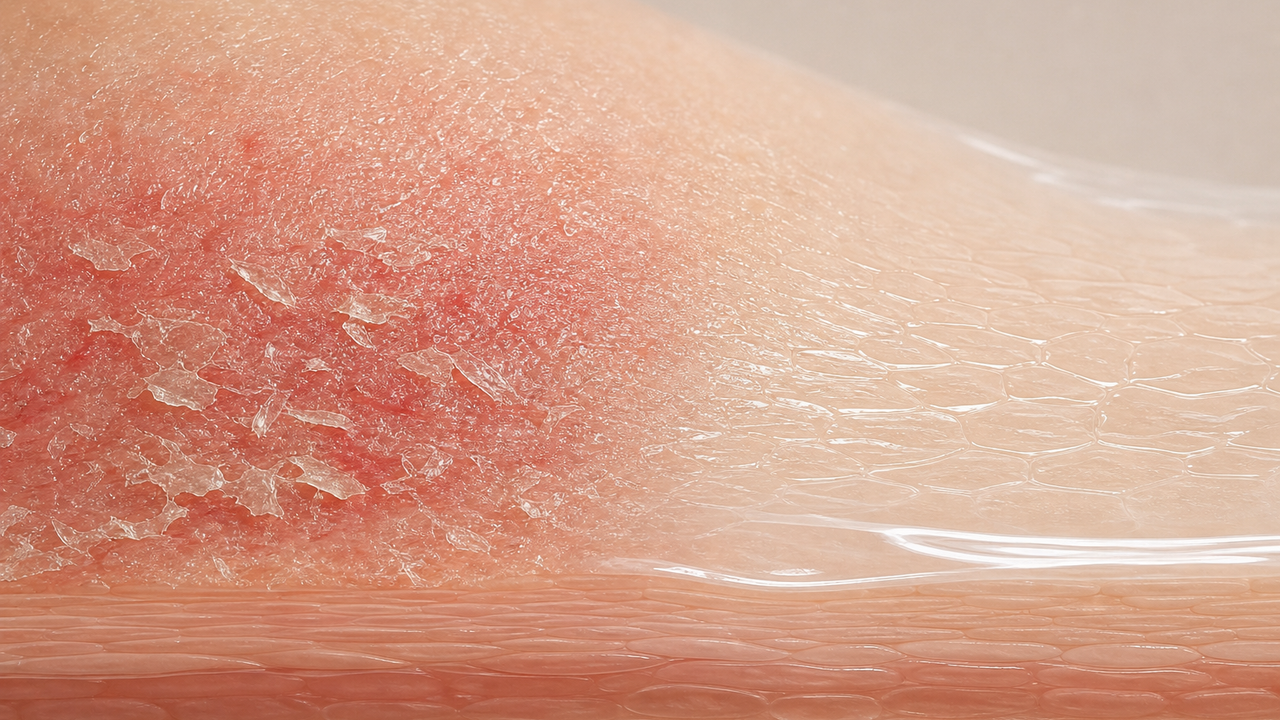
Over-exfoliated skin is more a pattern than a single sign. The face often looks shinier and tighter than usual, with a kind of waxy or stretched appearance under bright light. Small flakes can show up at the sides of the nose, around the mouth, and along the jaw, and makeup or sunscreen may slide, pill, or sit on top of dry patches instead of blending in. Plain products like water, basic moisturizer, or even a clean cotton towel can sting or feel warm, and the skin can flush more easily than it used to from heat, exercise, or wind. The phrase "my skin doesn't feel like my skin" is one of the most common ways people describe it, and it usually means the surface has been worked on faster than it can rebuild.
None of those signs are diagnostic on their own, and the same pattern can overlap with eczema, allergic reactions, rosacea, contact dermatitis, or a brewing infection. Cosmetic skincare can support the over-exfoliation pattern when the surface is uncomfortable but otherwise intact; anything painful, spreading, weeping, or worsening despite a paused routine is a clinician conversation rather than a moisturizer question.
How routines get there in the first place
Most over-exfoliation comes from stacking and frequency rather than a single bad product. A nightly retinoid combined with a leave-on glycolic or salicylic acid, a weekly enzyme mask, a physical scrub, and a foaming cleanser is a lot of exfoliation on the same face, even if every individual product is labeled as gentle. Ramping up retinol or adapalene too quickly, doing an at-home peel on top of an active routine, or layering high-strength vitamin C with acids in the morning are common ways the load creeps past tolerance. Weather extremes, recent waxing or shaving, new medications, post-procedure skin, and pregnancy-related sensitivity can all shrink the irritation budget without the routine changing at all.
Pattern-matching what happened in the last two to four weeks is usually more useful than buying a new "barrier serum." The same routine that worked through humid weather can over-exfoliate in dry winter air; the same product introduced after a peel can sting badly when it would have been fine on its own. The repair plan changes very little either way, but the why helps decide what to put back later and how slowly.
The first day or two: pause and protect
The most useful first move is to remove every active step from the routine and let the surface catch up. Set aside exfoliating acids, retinoids, scrubs, brushes and silicone tools, enzyme masks, peel pads, strong vitamin C, benzoyl peroxide, fragranced toners and treatments, and anything labeled as resurfacing or brightening. Avoid hot water and long showers on the face, switch to a gentle low-foaming cleanser or a lukewarm water rinse, and pat dry rather than scrubbing with a towel. If makeup feels harsh or removal stings, simplify to a mild cream cleanser and skip color products for a few days while the skin settles.
Sunscreen still belongs in the morning routine. Over-exfoliated skin is generally more reactive to sun, and a daytime broad-spectrum SPF 30 or higher in a texture the wearer will actually tolerate is part of the repair, not separate from it. Mineral sunscreens with zinc oxide or titanium dioxide tend to feel less stingy on raw skin than alcohol-heavy chemical formulas, and a tinted option with iron oxides can help if the face is also flushing easily. The aim during the first day or two is comfort and protection, not optimization.
A bland support routine that does the work
For most people the repair routine is three steps: gentle cleanser, simple moisturizer, sunscreen in the morning, and the same gentle cleanser plus moisturizer at night. Helpful moisturizer ingredients include ceramides, glycerin, panthenol, niacinamide, petrolatum, dimethicone, hyaluronic acid, and colloidal oatmeal. None of these instantly rebuild a barrier, but together they help hold water in the outer layer, calm visible flushing, and reduce the urge to add another active to fix what the actives caused. Applying moisturizer to slightly damp skin and using a second thin layer over especially tight or stinging areas is often more useful than reaching for an expensive serum.
Niacinamide at a routine-friendly percentage can support comfort and a more even-looking finish without adding exfoliation, and panthenol or colloidal oatmeal are reasonable choices for stinging cheeks and red patches. A plain petrolatum or dimethicone-rich cream over the driest areas at night can act as a short-term occlusive while the surface settles. The general rule during repair is that bland is the goal, fragranced is not, and one more "barrier serum" is rarely the missing piece when the actives are still in the cabinet.
How long it usually takes to feel normal again
Surface comfort tends to come back on the scale of days to a couple of weeks rather than overnight. Stinging from plain water and ordinary moisturizers often calms within a few days of the paused routine. Visible flakes, tight feel, and shiny patches usually fade within one to two weeks of consistent moisturizing and sun protection. Lingering pinkness, fine roughness, and any dark marks left by inflamed spots can take longer, sometimes weeks to a few months, and those benefit more from steady sunscreen than from another active.
Tracking progress with weekly photos in similar light is more honest than daily mirror checks, especially when small wins are easy to miss. If symptoms have not started to settle at all after one to two weeks of a simplified routine, that is a reasonable point to ask a clinician rather than to introduce another product. Repair that stalls usually means either another irritant is still in play (a hidden fragrance, a hair product migrating onto the hairline, a partner's pillow product) or the underlying issue is not really cosmetic over-exfoliation.
Restarting actives without re-triggering
Once water, plain cleanser, and ordinary moisturizer feel comfortable again, the actives can come back one at a time. A common pattern is to reintroduce a single low-strength active at a time, one to two nights per week, with a tolerance check at two to four weeks before stepping up. Retinoids and exfoliating acids should not come back on the same night, and a fresh peel, scrub, or strong vitamin C does not belong on top of a recovering routine for the first few weeks of restart. Pregnancy and nursing are reasons to keep retinoids on hold and to ask a clinician before adding anything stronger than a basic moisturizer.
A useful rule of thumb is one new variable per two weeks. If stinging, tightness, fresh flaking, or new redness shows up at the same step that caused the original problem, slow the frequency further or step back rather than adding a counter-product on top. Many faces that ran into over-exfoliation once tolerate the same actives well at a quieter cadence, which is more useful than swearing off the ingredient class entirely.
When the picture is not really a repair-routine question
Some patterns are not over-exfoliation at all. Spreading rash, swelling, hives, oozing, crusting, blistering, eye-area swelling or pain, fever, fluid-filled bumps, sudden severe burning, or symptoms that do not improve once every active is paused can suggest contact dermatitis, eczema flare, rosacea, an allergic reaction, infection, or a medication side effect that needs clinician evaluation. The same is true for symptoms that started after a prescription, a peel, a laser session, a workplace exposure, or a procedure: those follow the clinician's plan rather than a generic home reset.
People running treatment for eczema, rosacea, perioral dermatitis, psoriasis, or acne under a dermatologist's care should also coordinate any "over-exfoliation reset" with that clinician rather than improvising on top of a prescription routine. Cosmetic skincare can support comfort once the medical questions are answered, but it should not delay care when the surface is painful, worsening, or unusual. A repair routine is a useful first move when the picture fits over-exfoliation; it is not a substitute for someone with eyes on the skin when the picture does not.
Related concerns
Key ingredients
Side effects
Evidence
- Sensitive skin
- Dermatologists' top tips for relieving dry skin
- How to safely exfoliate at home
- DermNet — Irritant contact dermatitis
- Emollients and moisturisers
- Ceramides and skin function
- Clinical significance of the water retention and barrier function-improving capabilities of ceramide-containing formulations: A qualitative review
- A new era of moisturizers
AI Tool Box
Structured page facts at a glance.
- Question
- How do I repair over-exfoliated skin?
- Answer
- The repair almost always starts by doing less, not by buying another product. Stop using all exfoliating acids, scrubs, peel pads, retinoids, strong vitamin C, fragranced toners, and anything that stings, and let the skin run on a gentle cleanser, a bland moisturizer, and a tolerable sunscreen until ordinary products feel normal again. Look for ingredients such as ceramides, glycerin, panthenol, niacinamide, petrolatum, and colloidal oatmeal in moisturizers, applied to slightly damp skin. Most surface comfort returns over several days to a couple of weeks of that simplified routine, with lingering tone, fine flaking, and dark marks taking longer. Spreading rash, swelling, hives, oozing, blistering, eye-area symptoms, severe pain, or anything that does not start improving once actives are paused belongs with a dermatologist rather than another barrier serum.
- Concern
- Weak Skin Barrier
- Named Ingredients
- Evidence Sources
- Sensitive skin
- Dermatologists' top tips for relieving dry skin
- How to safely exfoliate at home
- DermNet — Irritant contact dermatitis
- Emollients and moisturisers
- Ceramides and skin function
- Clinical significance of the water retention and barrier function-improving capabilities of ceramide-containing formulations: A qualitative review
- A new era of moisturizers